AREAS. Revista Internacional de Ciencias Sociales, 43/2022
Social and environmental effects of mining in Southern Europe (pp. 53-65)
DOI: https://doi.org/10.6018/areas.493751
Managing miners’ health: occupational diseases, scientific management and workers’ life in the Italian mines of Peñarroya (1920-1950)
Francesca Sanna
Université de Reims Champagne-Ardenne
Abstract
The implementation of practices to protect miners’ health was slowly formalized in Europe beginning from the end of the 19th century. The legal pathway was equally long in all countries, especially in relation to the recognition of companies’ liability in the emergence of pathologies related to workplace morbidity . As there were no precise regulations and no medical agreement on the interpretation of certain diseases, health in the mine remained an ambiguous matter for mining companies, especially in relation with psycho-physical selection of workers and qualification of labour. In the interwar period, the problem of occupational health in the mines became more urgent, worsened by the introduction of scientific management and new extractive technologies. As showed by Paul André Rosenthal, silicosis became and it’s still today a global problem, both geographically and conceptually.
In this paper we focus on the case of Italian mines of Pertusola, the Italian subsidiary of the greater group Peñarroya, which became one of the biggest European mining and metallurgical corporations in the first part of the 20th century. At the crossroads between the value of health and that of performance at work, a space was opened for the development of practices, tools, measures, and techniques to act on both performance and occupational health, via the materiality of the human body. By the analysis of the firm strategy and initiatives, this paper aims at clarifying the transformation of occupational health in a managerial issue.
Keywords
Miners, occupational health, medical discourse, Peñarroya, 20th century
JEL codes: Ν33, Ν34, Ν54, Ν54
LA GESTIÓN DE LA SALUD DE LOS MINEROS: ENFERMEDADES PROFESIONALES, GESTIÓN CIENTÍFICA Y VIDA DE LOS TRABAJADORES EN LAS MINAS ITALIANAS DE PEÑARROYA (1920-1950)
Resumen
La
implementación de prácticas para proteger la salud de los mineros se
formalizó lentamente en Europa a partir de finales del siglo XIX. El
camino legal fue igualmente largo en todos los países, especialmente en
relación con el reconocimiento de la responsabilidad de las empresas en
la aparición de patologías relacionadas con la morbilidad laboral. Como
no existían normas precisas ni acuerdo médico sobre la interpretación de
ciertas enfermedades, la salud en la mina seguía siendo un tema ambiguo
para las empresas mineras, especialmente en relación con la selección
psicofísica de los trabajadores y la calificación de la mano de obra. En
el período de entreguerras, el problema de la salud ocupacional en las
minas se hizo más urgente, agravado por la introducción de la gestión
científica y las nuevas tecnologías extractivas. Como mostró Paul André
Rosenthal, la silicosis se convirtió y sigue siendo hoy en día un
problema global, tanto geográfica como conceptualmente.
En este artículo nos centramos en el caso de las minas italianas de
Pertusola, la filial italiana del gran grupo Peñarroya, que se convirtió
en una de las mayores corporaciones mineras y metalúrgicas europeas en
la primera parte del siglo XX. En la encrucijada entre el valor de la
salud y el del desempeño en el trabajo, se abrió un espacio para el
desarrollo de prácticas, herramientas, medidas y técnicas para actuar
tanto sobre el desempeño como sobre la salud ocupacional, a través de la
materialidad del cuerpo humano. A través del análisis de la estrategia y
de las iniciativas de la empresa, este artículo tiene como objetivo
aclarar la transformación de la salud ocupacional en una cuestión
gerencial.
Palabras clave
Mineros, salud ocupacional, discurso médico, Peñarroya, siglo XX
Códigos JEL: Ν33, Ν34, Ν54, Ν54
Original reception date: September 29, 2021; final version: March 4, 2022.
Francesca Sanna, Université de Reims Champagne-Ardenne.
E-mail: francesca.sanna10@gmail.com.
Managing miners’ health: occupational diseases, scientific management and workers’ life in the Italian mines of Peñarroya (1920-1950)
Intro
The implementation of practices to protect miners’ health was slowly formalized in Europe beginning from the end of the 19th century. The legal pathway was equally long in all countries, especially in relation to the recognition of companies’ liability in the emergence of pathologies related to workplace morbidity1. As there were no precise regulations and no medical agreement on the interpretation of certain diseases, health in the mine remained an ambiguous matter for mining companies, especially in relation with psycho-physical selection of workers and qualification of labour. In the interwar period, the problem of occupational health in the mines became more urgent, worsened by the introduction of scientific management and new extractive technologies. The increasing mechanization and the expanding use of explosives and drills raised the number of accidents and mortality rates, but also the incidence of occupational diseases like silicosis, strictly related to the increased volume of dust. In the interwar period, silicosis was considered the “king of occupational diseases”2, not only in relation to mining industry, but also in other industrial sectors like glass industry or pottery. As showed by Paul André Rosenthal, silicosis became and it’s still today a global problem, both geographically and conceptually.
In this paper we focus on the case of Italian mines of Pertusola, the Italian subsidiary of the greater group Peñarroya, which became one of the biggest European mining and metallurgical corporations in the first part of the 20th century3. During the interwar period, in a time of crisis, Pertusola adopted some measures of rationalization – time studies, organizational renovation, implementation of new technologies and labor evaluation techniques – which eventually became part of a more global strategy of managerial transformation of the firm4. Among the elements that were on that agenda, occupational health and safety became more and more urgent as the increasing rate of accidents, injuries and chronic diseases raised critically the compensation costs. The company had to take action and put its engineers and medical staff to work, in order to firstly find a solution to reduce those costs. The aim of this paper is to retrace and reconstruct the elements of this research and to show how the issue of occupational health and safety was first perceived and conceptualized as a problem with multiple aspects, such as medical, technical, economic, and social ones. This multiple conception of health eventually leaded to ambiguity and confusion on how to cope with injured or ill miners, and more specifically with their body. In fact, physical conditions of workers became an essential variable for labor performance evaluation and, in a time of scientific management implementation, labor efficiency was at the top of the agenda. At the crossroads between the value of health and that of performance at work, a space was opened for the development of practices, tools, measures, and techniques to act on both performance and occupational health, via the materiality of the human body. By the analysis of the firm strategy and initiatives, this paper aims at clarifying the transformation of occupational health in a managerial issue.
The Pertusola Mining and Metallurgical Company and its mines in Italy
The Società Mineraria e Metallurgica di Pertusola (Pertusola) was an Italian mining and metallurgical company founded as a subsidiary of the Société Minière et Métallurgique Peñarroya (SMMP) in Genoa in 1924, following the re-capitalization and headquarter change of the former Pertusola Ltd, which was acquired by SMMP in 1920. Pertusola had two main mining sites in the south-west of the Italian island of Sardinia, San Giovanni and Ingurtosu. The lattest was previously owned by the Société civile des mines de Gennamari et Ingurtosu, a subsidiary of Pertusola Ltd. Pertusola also owned a mining site in the north of the same island, Argentiera (which was acquired in 1923 by the absorption of Società Mineraria e Metallurgica di Correboi)5. The mines of Malfidano, always in the south-west of Sardinia, were later acquired in 1929, when SMMP absorbed the French Société Anonyme des Mines de Malfidano, which controlled also the smelting site of Noyelles-Godeault in France. In the later 1930s Pertusola acquired also other smaller mining sites in the same south-western region of Sardinia. In Italy, Pertusola owned also two smelting plants in La Spezia (in the north-western region of Ligury) and Crotone (in the south-eastern region of Calabria), but those industrial sites are not included in our study, focused on mining sites.
In Sardinia, Pertusola had an average mining workforce of 1500 people in the 1920s, which diminished to 600 in 1931 due to the mining crises related to Great Depression.
Table 1: Mining Workers in Pertusola Mining Company 1923-1931
|
Year |
Average number of workers |
|
1923 |
1,000 |
|
1924 |
1,200 |
|
1925 |
1,550 |
|
1926 |
1,800 |
|
1927 |
1,550 |
|
1928 |
1,250 |
|
1929 |
1,150 |
|
1929 |
1,000 |
|
1930 |
900 |
|
1931 |
600 |
|
1933 |
500* |
|
1935 |
1,500 |
Source: Rapport de Visite, San Giovanni, Mai 1931, Fondo Pertusola Piombo Zincifera, ASMM
Ingurtosu and San Giovanni mines are the largest mines of Pertusola, primary interested by the introduction of rationalization practices in the interwar period. Those mines have a unique technical and administrative direction. The same engineers are employed at both locations, and general director visited them periodically. Geologically and geographically, those mines show considerable differences. Ingurtosu is a filonian, quartzous and landslide lead and zinc deposit, exploited in two main pits separated by a hill (Gennamari and Ingurtosu). Those characteristics make it a difficult mine. San Giovanni is a lead-zinc deposit with fewer problems of exploitation. Geographically, Ingurtosu is situated in a particularly mountainous area, with little infrastructures, 15 km far from the nearest municipality (Arbus). As a chemical engineer noted in 1911, it would have taken one hour and a half to reach Arbus from Ingurtosu by horse-drawn carriage. Ingurtosu was not the best place for a miner to work and turnover was very high, so the company begin to build a mining village to keep the workforce more stable. San Giovanni, on the contrary, is very close to Iglesias, the main town in the area and the main mining distric on the island, and it is also very close to one of the biggest mines in Sardinia, called Monteponi. This makes the area particularly dynamic and well connected, with a road and a railroad. Both mines are surrounded by workers’ settlements, which the company tried to transform in a very company town in the case of Ingurtosu. In the case of San Giovanni, the settlement resembled more to a neighborhood, influenced by the attraction of Iglesias city center. Ingurtosu, situated at an altitude of 254 m, is the biggest of a few smaller settlements, distributed in proximity to the mining pits, partially isolated by the morphological structure of the area. Ingurtosu was inhabited by a growing number of people in the interwar period (650 in 1928) which grow up to 1800 people in 1952. The village was gradually abandoned after the 1960s, where Pertusola divested its activity to public companies which finally closed the mine in the late 1980s.
Part 1: Occupational health in the mine: accidents and diseases.
The problem of occupational health has frequently been related to that of safety and accidents. On the one hand this relation is the result of the legal system of compensation. In fact, in Europe, the compensation systems covering labor injuries usually included occupational diseases6. On the other hand, the companies considered occupational diseases and injuries on the same level: occupational diseases were considered as “accidents”, in the sense of events related to a pure contingency or unpredictability, a natural aspect of mining activity. Silicosis, for example, was called the “illnesses of the mine”7 or “miners’ fatigue”8, intended as an inevitable consequence of mining activity. For mining companies, the implicit attitude beneath this definition was not only fatalistic – accidents happen – but also discharging. Since accidents were considered inevitable, companies deemed that workers know and accept this risk as part of their job. The principle of acceptance was accentuated by the introduction of the technical regime of rationalization because mechanization and adoption of labor evaluation systems, such as time studies or piece rating, intensified the association between risk, virility, physical performance and social status related to remuneration9.
However, safety and health issues couldn’t be ignored or denied by the companies when they leaded to a sensible reduction of productivity or an increase of compensation costs.
In Italy, legislators had implemented some form of protection and compensation for workers since the end of 19th century10. However, this legislation was often poorly implemented in Sardinia, where Pertusola’s mines were located11. In 1912, the Inspectorate of Industry and Labour was created under the Ministry of Agriculture, Industry and Commerce in order to supervise the application of rules and codes, and to examine and solve legal conflicts related to labor. In 1919, a decree established the compulsory insurance for invalidity, associated with other laws related to retirement. During the Fascist regime, labor and welfare became issues of social control and totalitarian propaganda. From 1923 to 1933, all the institutions created for prevention, insurance and compensation were restructured under the sign of corporatism and regimentation. After the laws called “Fascistissime”, which abolished all the organizations related to political opponents to the regime, the fascist Labour Chart (1927) proposed a series of social security insurances, but article XXVIII stated: “It is the responsibility of workers associations to protect their representatives during administrative and legal prosecutions relating to insurance against accidents and social insurances”. In 1933, those remaining associations and insurances were incorporated in a new central organization called National Fascist Institute for insurance against occupational accidents (INFAIL). In the end of the 1920s, a few decrees began to take into account the protection against some of the most common occupational diseases, but not silicosis for example12. Only in 1943, after a spectacular increasing of judgments concerning silicosis compensation against many important firms, a new law imposed the compulsory insurance for silicosis and asbestosis, which compensated for a permanent invalidity over the 33% or for death. However, the regulation procedures for technical prevention were emanated only after the war. In Italy, at least until the first half of the 20th century, occupational diseases were considered a minor issue compared to the problem of safety, also because of the persistent ambiguity in legislation13.
In Pertusola’s mines during the interwar period the discussion about occupational diseases appeared more clearly after a series of initiatives against accidents, but a general debate about accidents, safety and health conditions in this mining area was quite developed since the end of the 19th century14. However, a statistic carried out on mortal accidents in all the mines of the region identified the worst rate increase (14%) between the decades 1900-1921 and 1922-194515. In this period, Pertusola, as many European mining companies, began to gradually introduce some forms of rationalization (time studies) and technological renovation16. However, the idea of complete mechanization of a mine was utopian, and the managerial efforts were more focused on how to mechanize human labour than the workplace as a whole. In this sense, taylorism was perceived more as an idea, a summa of principles: the “scientific” part of scientific management; other techniques of labour implementation like piece-rating formulas were considered the very practical tools to be used every day: the “managerial” part of scientific management. Mechanization became, in this sense, an option, that could have been implemented or not in relation to capital availability and the firm’s strategy. The introduction of this form of scientific management and those technologies strengthened, on the one hand, the problem of working conditions and dust exposure and, on the other hand, the idea of individual and personal responsibility of workers17. In Pertusola’s archives, two summary reports – one in 1927 about time studies and the other in 1933 about safety and dust exposure – indicated the same year 1923 as the moment in which the company began to introduce both scientific management and safety or anti-dust measures18. The management was aware that some sort of correlation between accidents and dust exposure, rationalization and mechanization existed. However, this suspicion did not open a critic to rationalization – as its principles were accepted as “scientific” - but it strengthened the idea of inadequacy of the workforce. In order to find the causes of accidents and diseases, Pertusola’s engineers looked more at collateral effects or at circumstantial factors, beginning from statistically quantifying the “visible symptoms”, such as accidents rates and workplace conditions.
Accidents and safety
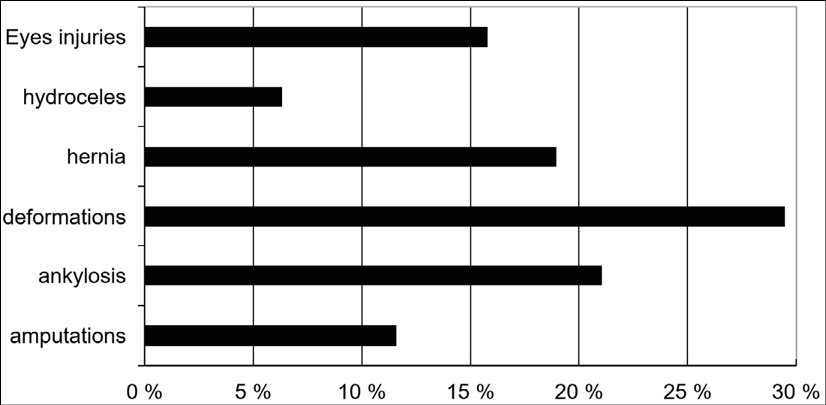
As it was more visible and, by its nature, more impacting on the daily schedule of mining activity, the problem of safety was perceived as more urgent by the management. The company’s statistics showed an increased number of small accidents affecting hands, legs and eyes of workers, like crushed fingers or broken feet, which demanded some days or weeks to recover. It was also noticed an increase of more serious cases, leading to partial or complete invalidity. Between 1927 and 1930, general accidents’ rate increased about 14% and recovering days’ rate from 2,0% to 3,3%19. In 1930 the higher rate of accidents was registered among haulers (37%), drillers and timbers (10% for each category). Some of those accidents could cause chronicle problems, affecting the general health conditions of the miners. For example, in 1933, in one of Pertusola’s mines, 37% of miners had physical injuries such as hernias, hydroceles, mydriasis, or other deformations, caused by iteration of particular activities or small accidents20. To this extent, as noted in many works about for Spanish workers of SMMP, the nature of this occupational risk is not accidental, but related to physical strain at work21.
Engineers became particularly attentive to the matter of safety and they began to notice the presence or the lack of safety measures when they commented the organization in other mines they visited. For example, in 1931, they visited some Peñarroya’s mines in Spain and they stated that, along with the great implementation of mechanization, no effort was made about safety, so accidents’ rate was very high22.
The increasing compensation costs and production loss, considered as consequences of accidents’ rate, forced the company to take action. A campaign for safety was ordered under the name of a “crusade23” against accidents. This lexicon reveals an attitude of authoritarian paternalism, even assuming the tone of a war (a holy war). As a first result, both accidents and recovery days were still increasing in number in the end of 1931, but the rate of serious accidents was decreasing24. The company thus considered workers incapable of adopting the right behavior25 and addressed them with the word of honor and shame, stressing personal responsibility. Beneath this paternalistic and moralistic discourse, was the issue of compensation costs26. In 1930, when the company published a list of adopted safety measures, it was clear that future serious accidents would have been considered as individual and personal responsibility of the workers27. The main principle of this politics was that: “for mining managers, it’s a duty to try diminishing the accidents’ rate with any mean, bur for miners it’s also a duty to avoid injuries”28. The company director published, some years later, an essay about mining accidents and safety in which, recalling many “true stories” from his personal experience, he concluded that the biggest danger for miners was their inability to calculate the risk of their actions29. The same warlike and paternalistic attitude appeared later in relation to the problem of dust.
Dust, silicosis and other occupational diseases.
In the first part of 20th century, surveys and studies found in Pertusola’s archive discuss the most popular thesis on silicosis, following the international debate about “miners’ consumption” in South Africa30. Firstly, conceived from an etiological point of view – for which hygienists linked a pathology to an activity or a substance – a medico-legal conception of dust related diseases prevailed at the beginning of the 20th century, not without political and social struggles in various European countries. Conceived as “occupational”, those diseases had to be treated by specific legislation, imposing on companies to adopt insurances and to compensate workers for health damages. However, the implementation of those laws was slow and uneven. In Italy, many medical surveys were published in 1930s about silicosis in different industrial sectors, contesting in particular the idea that silicosis was a variant of tuberculosis31. It is notorious that, at that time, silicosis was frequently described as tuberculosis. Silicosis symptoms can be easily mistaken, but the systematic diagnosis of tuberculosis was influenced by a “calculated bias”32 of mining companies, which acted in the process of knowledge making by introducing elements of uncertainty (criticism, doubt), related to the “regimes of imperceptibility” of diseases33. In fact, as tuberculosis was not considered an occupational disease, but a “personal ailment”34, related to individual habits and living conditions, companies were not responsible and they did not had to compensate workers. This strategy was part of a socio-political negociation in which a consistent part of the debate frequently resulted in minimized or contradictory compromises, creating a favorable terrain for the spreading of a auto-absolving discourse35. Silicosis was officially recognized by a ILO’s convention in 1934, but national legislation had a variety of regulations and procedures that sometimes limited the legal recognition of the disease36. In 1930, in the same year of Johannesburg conference about silicosis, the Italian Minister of Corporation supported the publication of an essay in which it was stated that dust was not pathogenic. Consequently, no intervention nor insurance had to be implemented for those industrial activities affected by dust exposure37.
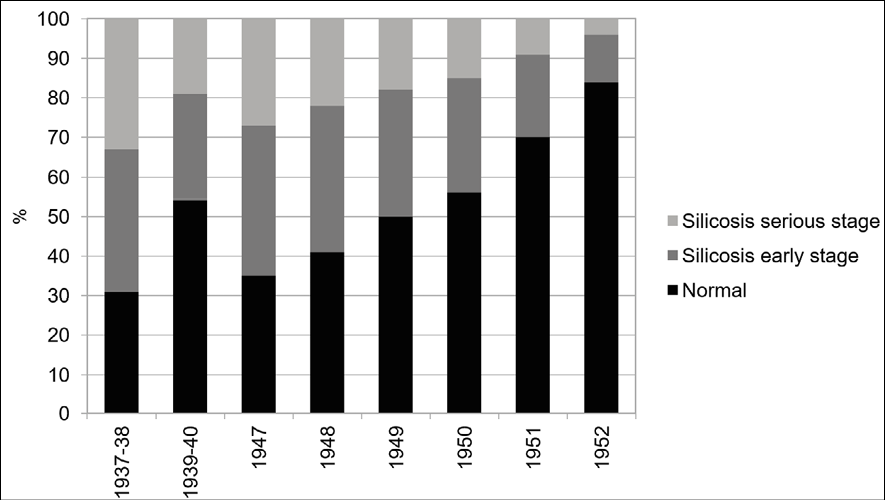
During the 1930s, a growing number of reports on dust and dust exposure appears in Pertusola’s archives. The need to implement mechanized operations provided the first motivation for studying environmental working conditions. At that time, scientific management ideas and practices were introduced more widely and, with the increasing of mechanization, labour organization became the core of a strategy centered on efficiency and productivity. The link between dust and silicosis was explicit in Pertusola’s reports, in which company’s historical “fight” against dust was put in direct relation to “the elevated disease rate among drillers”.38 Moreover, according to the company, only drillers could contract silicosis39. However, in two surveys carried out in 1936 and 1937, data showed that only 31% of miners were not affected by silicosis and that 33% had silicosis at serious stage40. Those data referred to miners working only underground and in ore washeries, not to the entire workforce. The same studies made clear that every miner exposed to dust could develop silicosis, but the company did not admit this conclusion until 1954, and not even explicitly41.
Studies were made also on the environmental conditions, showing an increasing number of dust particles in the air and a dangerous level of humidity, because of the lack of ventilation42. Until 1930, the most used anti-dust technology was perforation with water injection, which Pertusola introduced in 192343. However, after new findings about the solubility of silica, discussed during the Johannesburg Conference in 1930, water injection was replaced by previous technologies: aspiration devices and individual masks. Pertusola introduced some solutions, sometimes poorly crafted, such as fans for ventilation and other devices, or as to cover the pneumatic drill with a sack made in textile. The adoption of technological solutions such as aspiration devices and general fans suggests that dust was considered as an element of environmental disturbance: dust problem was related more to the workplace and labour productivity rather than to occupational health. Studies conducted by air sampling with a koniometer revealed that the ventilation system did not solve the problem of dust. The management decided to try some anti-dust mask, but they were not efficient: they didn’t absorb enough particles and they were uncomfortable in some cases, especially when the driller had to lay or to slither down in the narrow space between two fronts. They finally came to the conclusion that it was more convenient to create their own mask, which was finally adopted in 193444. According to the data, Pertusola’s mask absorbed 60% more of particles than other available masks and the filter box – the most uncomfortable part of the device – was separated from the facial mask and hanged to a belt or to external supports. After having equipped their drillers with this new mask, the company stated that every possible solution for diminishing dusk exposure had been adopted. The daily fight against dust was considered as a matter of personal responsibility and individual behavior of workers. In this sense, among the underground rule document, the only prescriptions related to health concerned anti-dust masks and nutrition (it was forbidden to eat underground and to drink from other people’s canteen)45. According to the sources, the only medical measure adopted before the war was x-rays surveillance, with periodical exams on workers (every year of every six-month depending on the exposure risk related to the tasks) to detect any deterioration of lungs, a possible symptom of incoming silicosis.
In the 1940s, the most common anti-dust measures at that time were still anti-dust masks: in 1953, the company doctor Emilio Pisano, who was a medical assistant in 1933, stated that the anti-dust mask developed in the 1930s was “very far from representing an effective protection for miners”46. He also recalled that the company decided to move miners with silicosis at serious stage on the surface and to change their tasks. It’s not specified if they have been compensated for the salary loss related to the less remunerative surface jobs. In 1939, the situation seemed ameliorated: underground and in the washeries, 54% of miners were not affected by any form of silicosis and no one had it at serious stage. However, no data were produced about surface miners, where the worst cases had been moved. A new labour organization system was also introduced, with shifting teams in the areas with the worst dust exposure, but the medical staff considered this experience ineffective. In 1945 a report stated that the lack of workforce in the mines was due to the fact that miners were “terrified by silicosis”47.
Studies were interrupted during the Second World War, because of lack of resources and because of the slowdown or even the suspension of mining operations. New statistics conducted from 1947 to 1952 showed an increase in normal health conditions’ rate of miners up to 84% and a decrease of early stage or moderate cases of silicosis from 65 % to 16%. However, the population of workers had changed and also the techniques of medical surveillance. However, until 1947, if the medical service “didn’t have any adequate means to directly prevent or detect”, doctors were also convinced that “every other medical initiative, except for those to improve the general living condition of miners, has little of no effect on silicosis prevention”48. This statement recalls the conclusions of the essay published in 1930 under the patronage of Minister of Corporations, for which the socio-hygienic conditions of labour were more impacting than dust exposure in relation to the insurgence of respiratory diseases. After 1947, new medical controls carried out with the help of the ENPI (the national agency for occupational safety) allowed the medical staff to get more data, but they came to the same conclusion: the radiological control was the only practical tool and the only possible medical strategy to gather information about health conditions of miners and eventually to introduce preventive solutions. So, silicosis and other illnesses were not surveyed to find medical treatments, but to gather data in other to find technical or organizational solutions for limiting dust-exposure. For example, according to the company director, perforation with water injection was reintroduced in 1951 “according to the report of Dr. Pisano referring to the medical examinations of the post-war [the first world war nda] years”49. According to the doctor, after the introduction of water injection in the 1920s (abandoned in the 1930s) the increasing rate of silicosis cases was not due to water injection, but to a statistical bias. So, still in the 1950s, most common anti-dust (and anti-silicosis) measures were water injection and anti-dust masks, but only for certain categories considered the most exposed.
During the interwar period, the company’s statistics showed that at least 50% of the cases of “serious diseases” among miners were represented by silicosis patients. However, silicosis was not the only danger: anemia, saturnism, pneumoconiosis, tuberculosis and malaria were quite common among miners50. Serious diseases, such as tuberculosis and pneumoconiosis, affected an average of 7% of miners between 1931 and 1933, but these data concerned only the miners who lived in the company town, which represented a variable percentage oscillating from 80% (1932) to 50% (1933). Those reports reflect the ambiguity of using the term silicosis to simplify the discourse about respiratory diseases related to dust: engineers assumed it uncritically while, at the time, only a minimal definition was recognized, and not without troubled negotiations and compromises51. Pertusola’s medical reports evoke especially the insurgence of tuberculosis, which was considered “the worst enemy of a person affected by silicosis”. According to the sources, the company always took in charge the hospitalization in sanatorium for miners affected by tuberculosis and, from time to time, the prophylaxis for malaria. The company also had at least two hospitals, located near its two main mining sites which was dedicated to the care of injured miners, and eventually their families52. However, it is to note that no initiative, or at least any discussion, concerning other diseases than silicosis appears in internal reports of the company, except for sporadic citation or statistics. Those diseases other than silicosis were treated separately, with a different strategy, more paternalistic, and in a different space, outside and not inside the mine. Silicosis, on the contrary, was conceived “technically”, as consequence of dust production and as a consubstantial condition of mining activity and labor management. In that sense, it became a matter of discussion for engineers and technical staff. However, anti-dust prescriptions for miners were considered a problem of “hygiene”53 and they were related to their individual and daily behavior at work, and especially on wearing, cleaning and manipulating the anti-dust mask. This ambiguity reflected the complexity of the international debate about silicosis, and the perception of it as an “epidemic”54 globally extended to mining industry55, but also fragmented by national legislation and denied or minimized by mining companies in the attempt to discharge from corporate liability.
Part 2 Test, select, control: scientific management and paternalism in and outside the mines
Launching the crusade against accidents in 1933 - “which is part of rational organization”56 - Pertusola also improved the activity of what was called “psycho-technical bureau”, a branch of the technical office57. The aim was to develop a system of selection for suitable candidates to hire. In fact, according to company statistics, a third of the total amount of accidents occurred because of workers incompetence, which was perceived as a consequence of a lack of training, but also of general ineptitude. Enlarging the core principle of rationalization (quantification), the management was convinced that it was possible to elaborate a scientific method for selecting workers on an analytic basis, associating biometrical data with the characteristic of mining tasks (qualification). This initiative was quite in line with the development of some branches of occupational medicine at that time. The interwar period could be considered the golden age of psycho-technique, a discipline at the crossroad of ergonomics and experimental psychology, both developed since the end of 19th century when biometric paradigm and anthropometry became the core of new tools for categorizing criminality and conceptualizing a new form of social control58.
Scientific management of health: medical data and labor evaluation
This shift in medical practice was accentuated in relation to selection and qualification processes, for which Pertusola developed a special branch of the technical office, in charge of elaborating a series of evaluation tools. The medical staff and the technical analysts of Pertusola began to cooperate, sharing data and information about workers’ medical profiles, in order to elaborate the selection criteria. For the medical staff this collaboration was a consequence of the lack of resources for medical initiatives59. The scope was to provide data for improving the efficiency of selection procedures, which, they thought, would have eventually ameliorated the occupational diseases’ rate. In fact, the increase of silicosis in the 1930s had been put in relation with the initial lack of control on medical conditions of candidates. So medical staff accepted to be “associated with the technical office which was carrying out quantitative and qualitative examinations of dust exposure in order to search a suitable solution to protect workers”60. Moreover, as many illnesses were considered discriminatory for hiring, medical staff could have help detect them and facilitate the selection process. The medical and psycho-technical examinations were compulsory for hiring, as stated in the general regulations61. So, selection was intended as a practice to solve the problem of occupational health by evacuating any critical case upstream. As we noticed above, no disease except for silicosis was treated in Pertusola’s internal reports, at least in the known archives. Among those illnesses, respiratory deficiencies, tuberculosis, syphilis, and alcoholism were listed all together as “symptoms that reveal a perceptible reduction of labor efficiency”62. To protect workers was the ultimate purpose for medical staff, but it was not the same for the technical staff and in some cases doctors were influenced by the efficiency discourse. So, if medical criteria were used to accelerate selection processes, technical criteria, such as efficiency, were the core of psycho-technical studies.
The collaboration produced many statistical studies based on the correlation between workers’ medical profiles, their job type (characterized on a qualification scale) and their performance rate, quantified with Bedaux evaluation system, which provided a sample for the new scales63. On those bases, the cabinet elaborated the selection criteria based on a score system, for which different tasks were characterized by a general score and by more detailed partial scores, related to biometric and psychological parameters. The cabinet also developed the psycho-technical tests for the evaluation of candidates. In those tests, workers obtained a numeric score which indicated the aptitude level. The correlation was implemented by an equivalence scale, associating the score to a job category, and it was elaborated exclusively by technical analysts under the supervision of engineers64. The use of Bedaux system as a sample for selection scales is particularly important to understand the strategy of the firm: it represents the attempt to reduce every aspect of the industrial production to the same evaluation technique, or the same metrology, and it reveals the pervasive power of scientific management as a transformative idea or a “mental revolution”65.
In Pertusola’s mines, health underwent a process of quantification and standardization, or evaluation, becoming a source of data for biometrical statistics, eventually used to elaborate selection criteria and tests. Data were transferred from medical staff to engineers and analysts by the creation of an archive of medical records66. In other words, those studies were performed with the aim of considering the technical and economic effects of the miners’ health rather than health as such. When those data suggested the emergence of generalized respiratory disorders, comments focused more on statistical errors related to the workers’ “careless behavior”. At the same time, the engineers introduced moral judgments to seek a plausible explanation for some “anomalies”. For instance, the good respiratory parameters of less performing workers were considered biased by “laziness”: they didn’t work hard enough. Health issue underwent the control of the technical staff, officially becoming a technical problem, to be solved with managerial solutions in the new rationalized organization of labor and workplace. Once the selection system set, the company continued to carried out its safety “crusade” and studies on dust, but with the aim of collecting data and implementing that system. Occupational health finally became more a matter of management than of medicine.
From the company point of view, every possible measure for prevention was appointed: the process of selection was the upstream solution and, for some workers, the distribution of special safety devices completed the anti-dust preventive system. If, after that, a miner injured himself or contracted some diseases, responsibility was his67, personal and individual. As a result, the company solved both the problem of liability and social control of workers. In fact, biometrical data became the core of the evaluation process (quantification and qualification) which eventually leaded to identification and disciplinarisation of labour via the materiality of the workers’ body. Health conditions in general, and not only occupational health conditions, became variables of labour performance, so they had to undergo the same systems of management and surveillance of other variables, like speed, rhythm, or technical skills. This leaded the company to extend his managerial attitude to every variable that could have interfered with workers’ health as a general state of human body and psyche, so to workers living conditions and private life. The intervention in private life, as a classic paternalistic act, was not new nor original for Pertusola, since the company had built and controlled a company town for at least 40 years. What was new was the transfer of managerial principles and tools in the classic paternalistic discourse and the turn of hygienist propaganda and initiatives in a more general “rationalized” strategy. In this sense, an occupational disease like silicosis, perceived as a substantial and inevitable diseases related to mining activity, was no more considered as a disturbing element to control, but as an integrated variable to manage.
The paternalistic approach to occupational health: disciplinarisation and personal responsibility
In Pertusola’s mines, engineers and managers have always been aware of the benefits of paternalism in terms of social control of workforce and they were inclined to imagine themselves as regulators of the “irrational” life of the workforce. The attempt to control workers private life is a well-known industrial practice since 19th century and, as Louis Reybaud cleverly noticed in 1874, mining companies always tried to “rule the families”68. In the 19th century those firms were some of the largest in terms of capital, investments and workforce employed. Their paternalistic initiatives, like the edification of company towns, aimed at creating a socially and culturally homogeneous workforce, dependent and sometimes truly loyal and emotively attached to the patronage. The social and economic scope of company towns was sustained by the hygienist discourse that developed from the 19th century, inspired by the work of Pasteur. Hygienist theories postulated a strict relation between living conditions and health. In general, it was stated that an improvement in the quality of housing or urban environment could have leaded to ameliorate the general health of the whole society. Industrial paternalism was deeply influenced by those ideas, for which living conditions influenced substantially the quality of men and, less frequently, women at work. However, there was no general agreement on practices and methods, nor on how to evaluate the benefits69.
Pertusola began to equip its mines with buildings and services for workers, like shops or leisure centers, since the end of the 1890s, but the situation was very different from mine to mine, depending especially on the environment and the proximity of urban centers. The more the mines were isolated, the more the company town was developed and the company control was powerful70. The process of creating towns or neighborhood was gradual: at the beginning, investments were not particularly extended and, as a results, mining villages were only a bunch of simple houses that resembled more to barracks71. Miners did not live stably there and did not move with their families. Later, and in the case of more isolated mines, the company began to develop more extended company towns, adopting also more clearly an attitude of control and surveillance. This control was typically materialized by rational urban planning and architectural style of housing, in order to impose a hierarchical idea of society by the power of authority. This authority was legitimized not only by economic power, which allowed mining company to invest in such urban projects, but also by a cultural one, related to the identification of company administrators, managers, and engineers with a civilizational principle of the bourgeois society72. The first purpose of paternalism was to regulate public and social aspect of miner’s life, in terms of organizing social relations and moral behavior, in order to help introducing the industrial discipline of time and hierarchy73. At the same time, the company intervened in more private aspects of miners’ life, related to family, individual identity and material existence, with the implementation of control on bodies with a hygienist propaganda, carried out with various acts of intrusion in the personal sphere, for example the inspection of houses and the regulation of nutrition habits74.
In the beginning of 20th century, the development of scientific management practices and ideas marked a turning point in how paternalistic practices were perceived in relation to firm strategy. Labor evaluation leaded Pertusola’s engineers to focus on the problem of labour efficiency, which identified effort and fatigue as key elements. While the workers’ body became the core of evaluation practices, the heritage of hygienist ideas suggested a link between psycho-physical profile and living conditions. Living conditions and private habits, like free time activities or diet, were considered as primary factors in the emergence of such diseases, like tuberculosis, that were discriminatory for hiring or for those chronic illnesses that surged in consequence of injures or labour exploitation. As we have noticed, the company did not implement any measures for dealing with or healing those illnesses, except for healing injuries in the hospital or sanatorium. Only malaria was treated with a particular attention75. Prevention and treatment were usually relocated in the private space of miners’ life and treated with a paternalistic display of different initiatives, such as the publication of periodical journal with sanitary and safety prescription for miners and their families76. More generally, the company had always considered private life as an influential factor on workers’ health conditions, which could have been a substantial condition of performance at work, but there was not a real attempt to quantify this impact. Conversely, along with the introduction of scientific management, engineers began to consider living standards and private habits as a quantifiable variable of labour performance evaluation. Paternalistic initiatives were rationalized and underwent to a logic of total evaluation, in which every aspect of an individual could have been quantified.
To this extent, private life became a space to regulate for efficiency purposes: home was intended as a space of relief for fatigue accumulated at work, in continuity with the space of the mine. Assumed as a stage of the productive cycle, home hosted the rest-time for energy recovery, to then constantly replicate the performance. In consequence, home became a space for the reproduction of energy efficiency. In that regard, women, wives and daughters of miners were targeted by paternalistic initiatives aiming not only at profiling the social gendered role of the good woman/wife/mother, but also at including family in the general labor efficiency strategy of the firm77. In this sense, family background and living conditions were considered not only influential variables of workers’ performance, but also quantifiable factors for their evaluation. For example, some Pertusola’s statistics put in relation labour productivity with family status, arguing that workers with a family were more productive than single ones by a statistical correlation. This language gave the impression of reducing the human factor to a mathematical scale and, finally, of being able to predict labour efficiency level by private background checking78. The company thus decided to give incentives and better houses to those miners with family in order to attract more of them instead of single miners. This choice increased the economic and social discrimination of single miners, who already lived in common housing, architecturally organized in a sort of panoptic enclosure. Those houses were also frequently inspected by the company director, who used to write his comments, impressions and suggestions in the local periodical, putting their private space into a public debate. Moreover, beginning from 1938, in order to comply with a new fascist law imposing “tax on single people”, Pertusola produced a list of single miners, with information about their age, birthplace and specific job in the mine79. The list identified and quantified a group of people who were not only morally stigmatized by the political regime, but also marginalized by the mining company because of a statistical correlation between family status and labour performance.
Observations on miners’ diet correlated with their economic and family status were legitimized by the principle for which unsatisfactory performance was due to the private misconduct of the worker or his family’s one, because the company assumed having evacuated the problem of ineptitude upstream, via the techno-medical selection process. The same logic implied that accidents and diseases occurred because of individual negligence in regards of safety in the mine and of personal health in private life. Therefore, these studies helped to justify a control on family, and the development of what might be considered as a sort of managerial paternalism, whose techniques were consistent to rationalization, and strictly related to the efficiency-gain strategy of the firm80.
Conclusions
During the interwar period, mining companies changed the way in which the issue of health and safety at work was taken into account, while they began a restructuring process of practices and strategies influenced by scientific management principles. The issue of health and safety is perceived by the firm as a legal and economic issue, linked to insurance and compensation. Accidents and occupational diseases affect the operating costs and, in the long term, the performance of the firm. However, the consequences of accidents and diseases also affects production on a daily basis but, in the absence of legislative obligations, prevention is not perceived as a company responsibility, but rather as an altruistic and philanthropic action in favour of workers. Prevention is mostly materialized in paternalistic acts and it is, for the most, evacuated upstream (through safety propaganda), downstream (compensation or medical treatment in the company’s hospitals) our outside the workplace. Influenced by hygienistic theories – which assessed some traditional paternalistic attitude – mining companies were inclined to consider health and safety as a consequence of personal behaviors, and to relocate preventive initiatives in the private space of miners’ life. The investment in day-to-day prevention of occupational risk (in which illnesses and accidents are included in equal measure) mainly concerns individual devices, both technological (dust masks) or organizational (rules of conduct). Safety regulations thus identify a managerial attitude that places the problem on a technical level and evacuates all the uncontrolled elements towards the personal and individual responsibility of the worker. The case of Pertusola mining company provides an example of how the introduction of scientific management could operate a managerial re-coding of the firm strategy and practices about safety and occupational health. In fact, with the introduction of rationalization, the problem of health and safety at work is no longer conceived as only a disciplinary or medical problem, but as a problem of labour performance, producing a shift from a medical to a managerial consideration of the individual psycho-physical factors. Assuming the traits of a factor or a variable affecting performance at work, health and safety are assessed and quantified in terms of potential and individual risk on the basis of the correlation between the psycho-physical characteristics of the worker and the specificity of the task. To this extent, the expansion of managerial thinking to all aspects of firm organization could also impact paternalistic practices and pretend to model workers’ private life for reproducing work efficiency. Finally, the principle of assessment and prediction in a preventive perspective is not applied to the risk in itself, but to the risk related to the individual, maintaining the assumption that the risk is inalienable to the job. Statistics identified a sanitary issue related to dust and, more generally, to the technical and environmental work conditions, but they provided a psycho-physiological representation with a managerial aim, not a medical one. Moreover, those statistics, based on medical data and workers profiles, where elaborated by analysts and engineers, and not by doctors.
The fact that there was no clear normative framework in regard to occupational diseases allowed these evaluation practices to emerge and, along with technical tools, to measure and to quantify health and safety according to certain technical criteria or ranking categories. Engineers, who took advantage of the scientific and technical knowledge of the time, appeared sometimes interested in understanding how the disease impacted the human body, but at the same time they were not interested in looking into the causal relationship between the disease and the specific organizational aspects of mining activities. What was at stake was the possibility to fully carry out the rationalization projects, with maximum efficiency and profitability. In a perspective of a technical and technological challenge, elements such as accidents and health issues were viewed as disturbances or obstacles to manage. The information about miners’ health and safety we get from these sources is distorted by this perspective, but they allows us to perceive, on the one hand, the transformations in the practical and conceptual behaviour of the mining firm and, on the other hand, how this managerial turn impacted miners’ life, in and outside the workplace.
Bibliography
Commissione parlamentare d’inchiesta sulla condizione degli operai delle miniere della Sardegna 1910, Atti della Commissione, II, Studi, statistiche e documenti allegati, Roma: Tipografia della Camera dei Deputati.
Commissione parlamentare d’inchiesta sulla condizione degli operai delle miniere della Sardegna 1911, Atti della Commissione, I, Relazione riassuntiva e allegati, Roma: Tipografia della Camera dei Deputati.
AUDIBERT, P. (1929): “Prevenzione razionale degli infortuni delle miniere di Gennamari Ingurtosu”, L’organizzazione scientifica del lavoro Rivista ENIOS: 709–712.
AUDIBERT, P. (1933): “L’azione di propaganda antiinfortunistica nelle Miniere della Società Pertusola in Sardegna”, L’Unione Industriale, 6.
AUDIBERT, P. (1943): Les accidents dans les mines métalliques et leur prévention, Paris, Liège, Beranger.
BALDASSARONI, A. & CARNEVALE, F. (1999): Mal da lavoro: storia della salute dei lavoratori, Rome, Laterza.
CARDINALE, A. (2005): Salute operaia. Le origini delle istituzioni per la protezione dei lavoratori in Italia (1896-1914), Archivio del Lavoro, Milano.
CASULA, D. (1986): “Le malattie dei minatori”, in Manconi, F. (ed.), Le miniere e i minatori della Sardegna, Silvana Editoriale, Milano: 233-236.
COHEN, Arón & FLETA Agustín (2011): “Un exemple de restriction des contours du “risque” au travail dans la pratique d’entreprise : la gestion patronale des hernies (Peñarroya, 1900-1950)” in Anne-Sophie Bruno A.-S. Geerkens, É. Hatzfeld, N. Omnès, C. (eds.), La santé au travail, entre savoirs et pouvoirs (XIXe-XXe siècles), Rennes, PUR: 123–143.
COOPER-RICHET, D. (2011): Le peuple de la nuit. Mines et mineurs en France. XIX e-XX e siècle, Paris, Perrin.
CUCCU, A. (2018): “Il laboratorio psico tecnico di Ingurtosu: un caso di organizzazione scientifica del lavoro nelle miniere della Sardegna”, Storicamente, 14/46. DOI: 10.12977/stor736.
FRONGIA, G. (1911): Igiene e miniere in Sardegna, Roma, Tipografia F. Centenari.
GIORDANO, A. (1913): La fisiopatologia e l’igiene dei minatori, Roma, Tipografia nazionale di G. Bertero e C.
HENRI, J. (2009): “Du paternalisme au managérialisme : les entreprises en quête de responsabilité sociale”, Innovations, 29: 149–168.
JULIEN, V. (2012): “Ramazzini n’est pas le précurseur de la médecine du travail [*]. Médecine, travail et politique avant l’hygiénisme”, Genèses, 4/89: 88-111.
KIPPING, M. (1999): “American Management Consulting Companies in Western Europe, 1920 to 1990: Products, Reputation, and Relationships”, The Business History Review, 73/2: 190–220.
KNOTTER, A. (2018): “Mining”, in Hofmeester, K. Van der Linden, M. (eds.), Handbook Global History of Work, Oldenbourg, De Gruyter: 237-258.
LAMANTHE, A. (2011): Les métamorphoses du paternalisme : Histoire, dynamiques et actualités, Paris, CNRS Éditions.
LAMPIS, Carla (2013): “Il periodico direzionale “Il Minatore” della miniera di Gennamari-Ingurtosu. Aspetti logistici, sanitari, sociali e tecnologici negli anni 1927-1929”, Ammentu. Bollettino Storico e Archivistico del Mediterraneo e delle Americhe (ABSAC), 3: 275-294. DOI: https://doi.org/10.19248/ammentu.94.
LAMPIS, Fernando (2017) Le miniere di Gennamari ed Ingurtosu nel panorama industriale Italiano Europeo «Piombo, Argento e Zinco» (1611-1991), S’Alvure.
LOPEZ-MORELL, M. Á. (2003): “Peñarroya: un modelo expansivo de corporación minero–industrial, 1881–1936”, Revista de Historia Industrial, 23: 95–136.
M.A.I.C. (1894): Studio sulle condizioni di sicurezza nelle miniere e nelle cave in Italia, relazione dell’ing. capo delle miniere E. Niccoli, Roma, 1894.
MANCONI, F. (1986): “L’economia e la società delle minier e dall’unità al fascismo”, in ID (ed.) Le miniere e i minatori della Sardegna, Cagliari, Consiglio regionale della Sardegna: 65-80.
MARKOWITZ, G. & ROSNER, D. (1991): Deadly Dust: Silicosis and the Politics of Occupational Disease in Twentieth-Century America, Princeton University Press.
IDs. (2017): “Why Is Silicosis So Important?”, in Rosenthal P.-A. Silicosis. A world history, Baltimore, John Hopkins University Press: 14-29.
MERCIER, L. & GIER, J. (2007): “Reconsidering Women and Gender in Mining”, History Compass, 5/3: 995-1001.
MOUTET, A. (2004): “La psychologie appliquée à l’industrie : un moyen de définition de l’aptitude et de l’inaptitude ? (de 1930 à 1960)”, in Cathérine Omnès, Anne-Sophie Bruno, Les mains inutiles. Inaptitude au travail et emploi en Europe, Paris, Belin: 83–101.
MURPHY, M. (2006): Sick Building Syndrome and the Problem of Uncertainty, Durham, Duke University Press.
MUSSO, S. (2004) : “Psychologie du travail et sélection de la main-d’oeuvre en Italie dans l’entre-deux-guerres”, in Cathérine Omnès, Anne-Sophie Bruno, Les mains inutiles. Inaptitude au travail et emploi en Europe, Paris, Belin: 102–124.
NELSON, D. (1999): A Mental Revolution. Scientific Management after Taylor, Columbus, Ohio State University Press,
PÉREZ DE PERCEVAL, M. A. (2006): “Minería e instituciones: papel del Estado y la legislación en la extracción española” in M. Á. Perez de Perceval, M. Á. López-Morell and A. Sánchez Rodríguez (eds.), Minería y desarrollo económico en España, Madrid, Síntesis: 69-93.
PERROT, M. (1979): “The Three Ages of Industral Discipline,” in Merriman, John (ed.), Consciousness and Class Experience in Nineteenth-Century Europe, New York, Holmes and Meier Publishers, Inc. p. 154.
PORRA’, R. (1993): “Infortuni sul lavoro nelle miniere sarde (1861-1886)”, in Kirova T. K. (ed.) , L’uomo e le miniere in Sardegna, Cagliari, Edizioni Della Torre: 65-80.
PROCTOR, R. & SCHIEBINGER, L. (2008): Agnotology: The Making and Unmaking of Ignorance, Stanford, Stanford University Press.
PUDDU, S. & LOCCI, F. (2004): “Completamento riordino e informatizzazione delle ricerche sui minatori caduti”, Minatori e Memorie, AMIME: 217–333.
RAINHORN, Judith (2014): Santé et travail à la mine. XIXe–XXIe siècles, Presses universitaires du Septentrion.
RAPETTI, Mariangela & TODDE, Eleonora (2018): “Gli ospedali minerari nella Sardegna dell’Ottocento”, in C. Villanueva Morte, A. Conejo de Pena and R. Villagrasa Elías (eds.), Redes hospitalarias: historia, economía y sociologia de la sanidad, Zaragoza, Institución Fernando el Católico: 245-256.
REID, D. (1985): “Industrial Paternalism: Discourse and Practice in Nineteenth-Century French Mining and Metallurgy”, Comparative Studies in Society and History, 27/4: 579-607.
REYBAUD, L. (1874), Le fer et la houille, Paris, Lévy.
ROLLANDI, Maria Stella (1985): “Il sistema Bedaux nelle miniere sarde della Pertusola (1927-1935)”, Studi Storici, 26/1: 69–106.
ROSENTHAL, P.-A. (2008): “La silicose comme maladie professionnelle transnationale”, Revue française des affaires sociales, 2-3: 255-277.
ROSENTHAL, P.-A. (2014) : “Préface. Les risques sanitaires dans les mines. Enjeux d’une histoire mondiale”, in Judith Rainhorn (ed.), Santé et travail à la mine. XIXe–XXIe siècles, Presses universitaires du Septentrion: 11-17.
ROSENTHAL, P.-A. (2017): Silicosis. A world history, Baltimore, John Hopkins University Press.
RUJU, S. (1999): “I mondi minerari in Sardegna e il caso dell’Argentiera”, in Musso, S. (ed.), Tra fabbrica e società. Mondi operai nell’Italia del Novecento, Milano, Feltrinelli: 313-380.
SANFELICE, F. & MALATO CALVINO, V. E. (1902):“Ricerche sperimentali sull’aria e statistiche sugli operai”, Annali d’Igiene Sperimentale, 12: 1-49.
SANNA, Francesca (2019): “La famille et l’OST: effets divergents de la rationalisation dans l’industrie minière de l’Europe du Sud pendant l’entre-deux-guerres.”, The Historical Review/La Revue Historique, 15: 57-90.
SANNA, Francesca (2020): “Évaluation technique et gestion managériale de la santé à la mine. Le cas des masques anti-poussière dans les mines méditerranéennes de la Société Minière et Métallurgique Peñarroya”, Actes du Colloque « Santé à la Mine », Lewarde, Centre Historique Minier du Nord et Pas-de-Calais, 4-5 Avril 2019, Edition Centre Historique Minier, 2020: 100-109 [english version: 207-209] URL: https://www.chm-lewarde.com/fr/en-acces-libre-les-actes-du-colloque-international-de-2019-sur-la-sante-a-la-mine/
SANNA, Francesca (2021, forthcoming): “Rationaliser le corps au travail en milieu minier : le cas de la Compagnie Minière et Métallurgique Peñarroya pendant l’entre-deux-guerres”, in Corps Au Travail : Performance, discipline et fatigue à l’épreuve du métier (XVIIe-XXe siècle), New Digital Fronteer.
THOMPSON, E. B. (1967): “Time, Work–Discipline, and Industrial Capitalism”, Past & Present, 38: 56–97.
TODDE, E. (2013): “Sicurezza, infortuni e scioperi nella miniera di Montevecchio nel corso del Novecento”, Bollettino Storico, Archivistico e Consolare del Mediterraneo, 3: 295-312.
TODESCO, L. (2018): “La sicurezza nelle miniere sarde tra Otto e Novecento: cosa ci raccontano le statistiche”, Storicamente, 14/32, DOI: 10.12977/stor722
VIGARELLO, G. (1978) : Le corps redréssé : Histoire d’un pouvoir pédagogique, Paris, J.-P. Delarge.
VINELLI, Marcello (1914): Note sull’industria, la mano d’opera e la legislazione nelle miniere di Sardegna, Cagliari, Società tipografica sarda.
1 Rainhorn (2014).
2 Markowitz, Rosner (2017: 14).
3 Miguel Á. López-Morell (2003).
4 Rollandi (1985).
5 Ruju (1999).
6 Rosenthal (2017: 2).
7 “Male della miniera” the original word “male” in italian has double significance of “illness” and “evil” or “bad thing”.
8 From spanish “fatiga de los mineros” that introduce the idea of consumption and exhaustion of the body. Pérez de Perceval (2006: 90).
9 Rosenthal (2014: 16).
10 In 1898, law n. 80 about accidents in industry - including mines, quarries and peatlands – introduced the idea of human error without dictating rules for prevention. Employers were forced to insure industrial workers (only some categories), but they were not considered responsible. In 1899, a series of regulations stressed the problem of accidents’ prevention (n. 231 for quarries and mines) and the general regulation n. 230 ensured the control of the worker’s physical integrity.
11 Manconi (1986: 71-72); Porrà (1993: 70-71); Todesco (2019); Todde (2013: 297-298).
12 The Royal Decree n. 928 (published in 1929 but later applied in 1934), extended the protection of industrial workers to occupational diseases such as lead, phosphorus or mercury poisoning, as well as to ankylostomiasis. The Royal Decree n. 1765 in 1935 created compulsory insurance for accidents and occupational diseases. This decree recognised all occupational diseases related to the processing of extraction as well as intoxication by carbon disulfide, but it did not mention other occupational diseases such as silicosis.
13 Baldassaroni, Carnevale (1999: 38-45, 55-60, 73).
14 Commissione (II, 1910), Commissione (I, 1911), Frongia (1911), Giordano (1913), M.a.i.c. (1894), Sella (1871), Vinelli (1914).
15 Puddu, Locci (2004: 329).
16 Rollandi (1985).
17 Markowitz, Rosner (1991).
18 The director of Pertusola’s mines, which authored those reports, began to work there also in 1923, so maybe this chronology was fabricated to get the merit of those initiatives. Settimo Rapporto Tecnico Generale (RTG), 1933, Fondo Pertusola, Rapporti, 1861-1966, Rapporti Tecnici Generali, 1930-36, 00616P – scaffale 20B – ripiano 1-2, dal I al X, Archivio Storico Minerario della Sardegna -Monteponi (ASMM), p. 22; Relazione sui cronometraggi, Paul Audibert, Fondo Pertusola, Bedaux-Cottimi, 1927-69, Bedaux, 1927-69, 00215P – scaffale 19B – ripiano 1-2, ASMM.
19 Terzo RTG, 1931: 64-65.
20 Elenco operai affetti da mutilazioni fisiche, imperfezioni ecc, Fondo Pertusola, Carteggio, 1923-56, 00765 – scaffale 21A – ripiano 3-4, ASMM.
21 Cohen, Fleta (2011).
22 Quarto RTG, 1932: 57.
23 Audibert (1929).
24 Terzo RTG, 1931, p. 64-65. In 1933, the director wrote in an article that this campaign reduced the accidents rate by 40% over 1000 working days but the data he indicated (104 accidents in 1930 and 27 in 1932) do not correspond to the data in the sources. Audibert (1933).
25 “The worst task is to train workers for this fight [against accidents], we need to make them more cautious and convince them that calculating on compensations is dishonest, that is a shame to injure themselves so frequently and that is honorable when they pass some years without being injured, when they avoid a comrade to be injured or when they save someone from a great danger” (translated from Italian) Secondo RTG, 1930: 50.
26 In 1933 the mine director pointed out “The fight against accidents is very opportune since we are now faced with a single insurance company which should not be given any pretext to increase premiums.” Settimo RTG, p. 39. The problem of compensation and the increase of insurance premiums was a concern for Italian industrialists since the 1920s. This phenomenon has been related to the introduction of mechanization. Baldassaroni, Carnevale (1999: 82).
27 Among this measures: the publication of a book containing safety measures, distributed among miners; the adoption of a safety police, surveillance and a system of fines ; distribution of safety equipment (not specified). Secondo RTG, 1932: 50.
28 Secondo RTG, 1932, p. 50. In the company general regulation document it was stated “The worker has to assume the duty of collaborating with the management in order to fight against accidents”. Regolamento, Carteggio, 1923-52, 00765 – scaffale 21A – ripiano 3-4, ASMM.
29 Audibert (1943: V).
30 The first medical qualification of respiratory diseases caused by dust particles in the air, known as « pneumoconioses » was proposed by Friedrich von Zenker in 1867. After « anthracosis » in 1838 (Thomas Stratton) and « siderosis » en 1867 (von Zenker), the term “silicosis” was used for the first time in 1870 by Achille Visconti, a pathologist, in an autopsy report on a quarrier, but it was Carlo Rovida who gave the first medical description of the disease in 1871. Baldasseroni, Carnevale (1999: 302).
31 In particular by Luigi Devoto. Baldasseroni, Carnevale (1999: 301), Rosenthal (2008). See also Cardinale (2005: 75-96).
32 Rosenthal (2017: 4).
33 Murphy (2006).
34 Ibidem.
35 Proctor, Schiebinger (2008).
36 Rosenthal (2017: 6).
37 Baldasseroni, Carnevale (1999: 303).
38 Settimo RTG, 1933: 22.
39 “drillers are the most affected by silicosis. We have not recorded any case of silicosis among other miners” Ibidem.
40 The first by Romano Vercesi, doctor at the sanatorium in Cagliari, published in 1936 and the second, a radiological study conducted by company medical staff under the supervision of Aristide Busi, doctor at Institute of Medical Radiology, Royal University of Rome, in 1937. Relazione sulla prevenzione medica della silicosi nelle miniere sarde della Pertusola. Convegno di Cagliari sulla sicurezza sul lavoro nelle minire, 1953, dott. Emilio Pisano, Fondo Pertusola, Carteggio, 1940-63, 00640P, scaffale 20B, ripiano 1-5, ASMM.
41 “from a recent study [...] it appears that the most exposed workers to silicosis are no longer the drillers, but the clearing workers and especially the pile drivers” (translated from italian) Rapporto di Visita, 17/11-7/12 1954, Fondo Crotone, Produzione Generale Sardegna,Visite a Miniere, 1929-1948, 00227, scaffale 21A – ripiano 1-1, ASMM.
42 Temperatura ed umidità cantieri Brassey 1a zona dicembre 1933, 3 janvier 1933, Fondo Pertusola, Rapporti Tecnici del Mercoledi Ingurtosu 1933, ASMM ; Misura dell’umidità nell’aria psicrometro, 27 décembre 1933, Fondo Pertusola, Rapporti Tecnici del Mercoledi Ingurtosu 1933. Some studies about dust particles and humidity in the mines of the region were conducted by local doctors in the beginning of the 20th century. Sanfelice, Malato Calvino (1911).
43 Settimo RTG, 1933: 22.
44 Sanna (2020: 207-209).
45 Regolamento, Fondo Pertusola, Carteggio, 1923-52, 00765 – scaffale 21A – ripiano 3-4, ASMM.
46 Relazione, op. cit.
47 Rapporto di Visita in Sardegna, 1945, Fondo Crotone, Produzione Generale Sardegna, Visite a Miniere, 1929-1948, 00227, scaffale 21A – ripiano 1-1, ASMM.
48 Relazione, op. cit.
49 Rapporto di Visita in Sardegna, Nov.-Dic. 1951, Fondo Crotone, Produzione Generale Sardegna, Visite a Miniere, 1929-1948, 00227, scaffale 21A – ripiano 1-1, ASMM.
50 Casula (1986), Ruju (1999: 330), Todesco (2019).
51 Rosenthal (2017: 6).
52 Lampis (2013), Lampis (2017), Rapetti, Todde (2018). Pertusola’s hospitals documents are not conserved in the ASMM. Their location is actually unknown and they are considered as missing. Some sparse information report that a first hospital was opened in Ingurtosu in 1907, and another in Gonnesa (near San Giovanni mine) in 1913. The first one was progressively equipped with radiological and chirurgical service, a laboratory for microscopic analysis and a pharmacy. From 1938, the radiology section was equipped with a “Gorla Sama” machine for detecting pneumoconiosis or other respiratory diseases.
53 Ibidem.
54 Baldassaroni, Carnevale (1999: 296).
55 Rosenthal (2017).
56 Terzo RTG, 1931: 51.
57 Rollandi (1985), Cuccu (2018), Sanna (2021, forthcoming).
58 Metrology of human body was also highly implemented in the military, for the selection of enlisted men to serve as soldiers. Vigarello (1978). For psychology in industry see especially : Aimée Moutet (2004); Stefano Musso (2004).
59 Relazione, op. cit.
60 Ibidem.
61 Regolamento, op. cit.
62 Relazione, op. cit.
63 Bedaux system is presented as a scientific evaluation of performance, which is reflected in a points-based remuneration system. These points are obtained through an assessment of the time taken to perform the task, calculated on the basis of a based on a standard that indicates the amount of work an average worker does in one minute. The evaluation, based on timekeeping, is intended to establish a standard speed so that, regardless of the type of work, the average worker can achieve the maximum amount of 80 B per hour. The determination of standard speeds depends on an empirical principle for which the optimal speed of execution of a task (the optimal ratio of time/efficiency variables) is related by ¾ to the average of the maximum (fastest) speeds recorded and set at 80 B/h. Yet the minimum standard speed, being ¾ of 80 B/h, is 60 B/h. The base salary is set at 60 B/h, above which we add the premium. About Bedaux system and Société Bedaux see Kipping (1999: 196-202).
64 For the detailed analysis of this tools: Sanna (2021, fothcoming).
65 Nelson (1999: 2).
66 Carteggio, 1940-63, 00640P, scaffale 20B, ripiano 1-5.
67 All the documents refer to male workers. On the one hand, this was due to the few number of women working in the mines (only on the surface), on the other hand, this absence reveals a statistical bias, related to the fact that engineers were convinced that only drillers or underground operators could contract silicosis. The same absence is even more relevant in the case of accidents: there is no statistical interest for a gender perspective on safety, but it is notorious that women have been victim of accidents in the mines. Mercier, Gier (2007).
68 Reybaud (1874: 203) cited in Cooper-Richet (2011: 56).
69 Julien (2012).
70 Knotter (2018: 250).
71 Rollandi (1985: 96).
72 Reid, (1985).
73 Thompson (1967).
74 Perrot (1979: 154).
75 Casula (1986), Ruju (1999: 330).
76 Lampis (2013: 290-293).
77 Rollandi (1985).
78 Sanna (2019: 65).
79 Lista Imposta Celibi, 1938, Fondo Pertusola, Carteggio, 1923-52, 00765 – scaffale 21A – ripiano 3-4, ASMM.
80 Lamanthe (2011), Henri (2009).
Source: Operai con lesioni, Fondo Pertusola, Carteggio, 1923-52, 00765 – scaffale 21A – ripiano 3-4, ASMM.
Figure 1. Workers’ injuries in the Pertusola mines (1933)
Source: Relazione sulla prevenzione medica, op. cit.
Figure 1. Workers’ injuries in the Pertusola mines (1933)